The Diabetic Foot
DIABETES, a chronic condition affecting an increasing number of people, highlights the crucial role of podiatrists.
The foot is the primary site of complications resulting from this disease, as 90% of hospitalized diabetic patients are admitted to treat a foot condition.
Diabetes can lead to neuropathic disorders (loss of sensitivity), arteriopathic issues (poor circulation of arterial blood), and serious podiatric complications.
Management by a podiatrist allows for the grading of podiatric risk, curative care, patient education, assessment of footwear, and the implementation of orthotic treatment (insoles) if necessary.
-
10 to 15% of diabetic patients still have to undergo amputation today when all therapeutic interventions have failed to halt the devastating effects of this disease.
-
It is therefore crucial to continue individual prevention efforts, which offer the best chance to optimize the quality of life for patients, alongside fundamental research on the disease itself.
Diabetic Gradation:
Grade 0:
No sensitive neuropathy.
Grade 1:
Isolated sensitive neuropathy.
Grade 2:
Sensitive neuropathy associated with lower limb arteriopathy and/or foot deformity.
Grade 3:
History of ulceration or amputation.
I. General Complications of Diabetes
The metabolic changes caused by diabetes schematically generate three major types of complications:
Neurological Complications
The involvement of peripheral nerves causes sensory and motor deficits, primarily affecting the nerves of the lower limbs (legs), with a distal predominance. The severity of nerve damage increases as it approaches the extremities.
Vascular Complications
Cholesterol deposits lead to a gradual blockage of large arterial trunks (macroangiopathy) as well as damage to small vessels (microangiopathy). Both phenomena cause arteritis predominantly in the lower limbs and impaired healing. Skin lesions heal poorly, creating potential entry points for germs responsible for infectious diseases.
Infectious Complications
The immune system of diabetic patients is weakened. Diabetics are more susceptible to bacterial infections and are also more vulnerable to skin and nail fungal infections. Furthermore, observed metabolic alterations reduce the effectiveness of antibiotic and antifungal treatments in these patients.
II. Impact of these Complications on the Foot
Consequences of Neurological Impairments
The vast majority of pathologies encountered on the diabetic foot originate from neurological impairments. Two types of lesions in the nervous system should be distinguished:
1. Sensory-Motor Impairments
These impairments of peripheral nerves, primarily affecting the lower limbs, constitute diabetic neuropathy, mainly of the polyneuritis type, leading to motor and sensory disorders
Sensory issues manifest as a gradual impairment of various forms of sensitivity. This includes, to varying degrees, deficits in touch perception, pain, paresthesia, or hypoesthesia. Sensitivity disturbances are also observed.
The onset of these sensory issues is often formidable because the foot, no longer well-informed about external threats or spatial parameters necessary for the fine adjustments required by the complex action of walking, is more susceptible to traumatic risks. This is especially dangerous in diabetics due to their impaired healing and vulnerability to infections.
2. Neurovegetative Impairments:
At the foot level, the vegetative nervous system (VNS), conveyed by motor and sensory nerves, is also affected by the disease.
Instead of evenly distributing arterial blood between the bone structure and the skin, it will favor the vascularization of skin tissues at the expense of the skeleton. This dysfunction leads to a disruption of the bone apposition/resorption system, responsible for diabetic arthropathies.
3. Osteoarticular and Cutaneous Impairments Induced by Neurological Degeneration:
Diabetic Arthropathies
The foot is particularly affected by this process of bone resorption, as it is maximal in the instep (tarsus) and the big toe, both vital for walking. The joints become red, swollen, and warm but are never painful. These are referred to as pseudo-inflammatory conditions.
Subsequently, deformities such as the collapse of the plantar arch due to tarsal involvement or toe dislocations (Charcot's foot) may occur.
Radiological Signs:
Identification of areas of osteoporosis and bone lysis, as well as images of bone formations (osteophytes) such as heel spurs because resorption is associated with the construction of aberrant structures on the margins of any functionality.
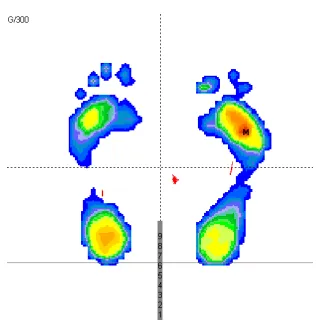
Cutaneous Consequences of Neurological and Osteoarticular Impairments on the Foot
The various bone deformities will alter the shape of the foot and the uniformity of its plantar supports. Pathological walking pressures will emerge, leading to the formation of calloused areas (hyperkeratosis) in areas of higher pressure. The lack of pain sensitivity often present at this stage of the disease, along with a lack of prevention, is often responsible for the transformation of these calluses into plantar ulcers.
In the absence of prompt intervention, these skin lesions progress towards chronicity as healing does not occur, and osteitis (skeletal involvement) is often a concern.
Blisters that may appear due to friction with shoes, though seemingly common, should be promptly treated under good aseptic conditions. They pose a risk of infection with the known dramatic consequences in a diabetic context.
Most of these pathologies occur at a stage of diabetic disease where the patient does not experience painful symptoms and, if not educated by healthcare professionals, may overlook a benign lesion that could ultimately have catastrophic effects. Simple yet rigorous care at the onset would have been sufficient for treatment.
Consequences of Arterial, Osteoarticular, and Cutaneous Disorders
Associated Cutaneous Lesions:
These severe lesions are caused by ischemic involvement of the arteries in the lower limbs, within the context of diabetic macroangiopathy. They result in a reduction of arterial blood flow to the foot, with a decrease or abolition of arterial pulses and cooling of the skin. Eventually, ulcers may occur, leading to toe necrosis and sometimes complicated by gangrene.

Other Cutaneous Infections
Superinfected Fissures
Fungal Infections.
The cutaneous, immune, and vascular alterations in diabetes also contribute to the development of fungal infections, manifesting as infections in the toes or interdigital spaces. It is crucial to emphasize the need for rigorous treatment, bearing in mind that the healing process may take longer than in a non-diabetic individual.
The diabetic foot is fragile, constantly at risk, and can lead to complications in the vascular, neurological, skeletal, and cutaneous aspects, with dramatic consequences for the patient's autonomy and survival.
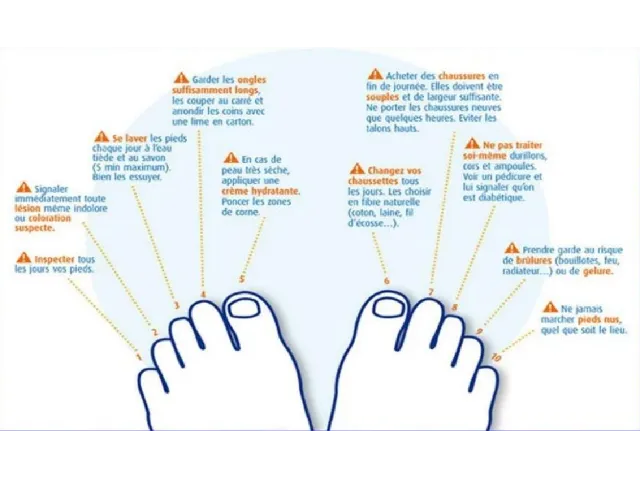
Regular monitoring and effective prevention fortunately help avoid many troubles. The foot plays a major role in the quality of life and health of a diabetic.
This subject is the epitome of the need to inform for better prevention and to prevent better for better relief.